

Cancer of the kidney is a common urological malignancy. There are over 13,100 people diagnosed with kidney cancer each year in the UK. Kidney cancer is more common in men than in women. It is the 7th most common cancer in the UK. For reasons that are not well understood, the incidence is rising and has increased by 36% in the last decade (1)
Nearly 2 out 3 people diagnosed (62%) are over 65 years old.
Kidney cancer is a cancer that starts in the kidneys. In order to understand kidney cancer, it helps to know about the normal structure and function of the kidneys.
About the Kidneys
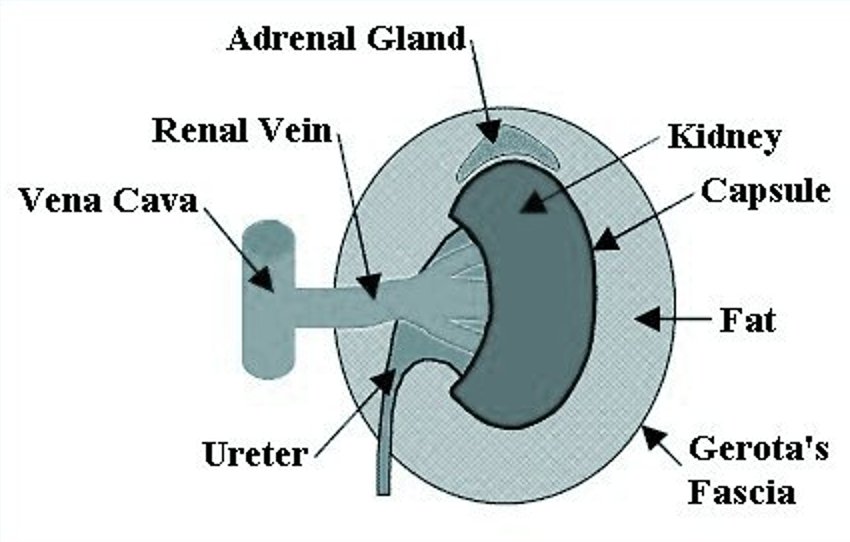
The kidneys are a pair of bean-shaped organs, each about the size of a fist and weighing about 4 to 5 ounces. They are fixed to the upper back wall of the abdominal cavity. One kidney is just to the left and the other just to the right of the backbone. Both are protected by the lower ribcage. The kidney is contained within a fibrous sheath called Gerota’s fascia. Within this fascia is a layer of fat that surrounds the kidney. The capsule is a thin layer that covers the outer surface of the kidney (analogous to the red external layer of an apple). The primary vein that drains the kidney (renal vein) merges with the vein that takes blood to the heart (vena cava). The term “renal” means pertaining to the kidney. An adrenal gland is located above each kidney within Gerota’s fascia.

The kidneys’ main job is to filter the blood and rid the body of excess water, salt, and waste products. The filtered waste products are concentrated into urine.
Urine leaves the kidneys through long slender tubes called ureters that connect to the bladder. Urine flows down the ureters into the bladder, where it is stored until urination.
The kidneys also help make sure the body has enough red blood cells. It does this by making a hormone called erythropoietin, which tells the bone marrow to make more red blood cells.
Although our kidneys are important, we actually need less than 1 complete kidney to do all of the functions discussed above. Many thousands of people are living normal healthy lives with just 1 kidney. Some people may not have any working kidneys at all, and survive with the help of a medical procedure called dialysis. Dialysis uses a specially designed machine that acts like a real kidney to filter the blood.
Understanding Cancer
Cancer begins in cells, the building blocks that make up tissues. Tissues make up the organs of the body.
Normally, cells grow and divide to form new cells as the body needs them. When cells grow old, they die, and new cells take their place.
Sometimes this orderly process goes wrong. New cells form when the body does not need them, and old cells do not die when they should. These extra cells can form a mass of tissue called a growth or tumour.
Tumours can be benign (non cancerous) or malignant (cancerous)
What is kidney cancer?
There are several types of kidney cancer, but most cases are ‘renal cell cancer’. This is sometimes called ‘renal adenocarcinoma’ or ‘renal cell carcinoma’ or ‘hypernephroma’.
Renal Cell Cancer
The most common type of kidney tumour is a fluid-filled area called a cyst. Simple cysts are benign and have a typical appearance on imaging studies. Simple cysts do not progress to cancer and usually require no follow-up treatment. Complex cysts do not have the typical benign appearance and may contain cancer. When complex cysts are present, the need for treatment is determined on an individual basis.
Solid malignant tumours develop from a cell in a kidney tubule which becomes cancerous. The cancer grows and forms into a tumour within the kidney. As the tumour grows:
- The affected kidney tends to become larger. In time the tumour may grow through the wall of the kidney and invade nearby tissues and organs such as the muscles around the spine, the liver, the nearby large blood vessels, etc.
- Some cells may break off into the lymph channels or bloodstream. The cancer may then spread to nearby lymph nodes or spread to other areas of the body (metastasise).The most common site of spread is to the lungs.
Renal cell cancers can be divided into several ‘sub-types’ by looking at certain features of the cells under a microscope. For example, most are ‘clear cell’ renal cell cancers, but some other types occur such as ‘sarcomatoid‘, or ‘granular‘ renal cell cancers. Knowing the sub-type of the cancer can be important as some respond to treatment better than others.

Other Types of Kidney Cancer
Some less usual types of cancer arise from other types of cell within the kidney. For example:
- Transitional cell (urothelial) cancers are cancers, which arise from transitional (urothelial) cells. These are cells which line the renal pelvis, ureters and bladder. Transitional cell cancer is common in the bladder, but in some cases it develops in the renal pelvis in the kidney.
- Wilms Tumour and Clear Cell Sarcoma of the kidney are types of kidney cancer which develop only in children.

Are there any risk factors for Kidney cancer?
Smoking
If you smoke then your risk of getting kidney cancer could be double that of a non-smoker. The longer you continue to smoke and the higher the number of cigarettes you smoke, the higher the risk becomes. But if you stop smoking then your risk of getting kidney cancer will probably fall. (2)
Being overweight
Obesity increases the risk of getting kidney cancer. ‘Obese’ means that your body mass index is over 30. Or more roughly, that your weight is at least 25% higher than the top of the range for your height. Being overweight causes changes in hormones in the body, particularly for women. It could be this change in the body’s hormone balance that increases the risk of kidney cancer. (3)
Nutrition
Apart from obesity, we aren’t sure what part diet plays in kidney cancer. There is a higher incidence of renal cancer in countries eating Western diets as opposed to China and Japan and other countries where a lower fat and more soya based diet is consumed. Therefore it seems as if eating large amounts of well cooked meat or having a high fat intake may increase the risk. People who eat enough fruit, grains and vegetables( particularly dark green vegetables) and limit intake of fats and calories may lower their risk of kidney cancer. These dietary guidelines can lower your risk of other cancers too , as well as heart disease. (4)
Kidney disease
People with kidney failure have to have their blood filtered by machine about twice a week. This is called dialysis. People having long term kidney dialysis have an increased risk of developing kidney cysts and these increase the risk of kidney cancer. The longer you are on dialysis, the greater your risk of kidney cancer. The dialysis itself is not directly related to the cancer risk.
High blood pressure
Some research studies have found a link between high blood pressure or high blood pressure medicines and kidney cancer. It is more likely that high blood pressure is the link, rather than the medications. High blood pressure is a known risk factor for kidney disease in general.(5)
Industrial Chemicals
Sometimes, hazardous substances in the workplace can increase the risk of kidney cancer. There is evidence that working with coke ovens or blast furnaces in the iron or steel industries increases kidney cancer risk.
Asbestos might also increase the risk of kidney cancer. People in a variety of occupations were exposed to asbestos in the past, including builders, car mechanics and shipyard workers.
Exposure to cadmium (a type of metal) and organic solvents, particularly trichloroethylene, may also be risk factors for kidney cancer. The risk if you work with cadmium is known to be greater if you also smoke. (6)
Other occupations that may increase the risk of kidney cancer include dry cleaning and the petrochemical industry.
Faulty genes
Some people inherit a tendency to develop kidney cancer. This is called hereditary or familial kidney cancer. The increased risk of cancer is related to an inherited faulty gene. Changes in the DNA that makes up the gene make it behave in an abnormal way and this can increase your risk of cancer. Scientists are finding out which genes carry these mistakes in the DNA. In the future this could help doctors predict who is at risk of getting hereditary kidney cancer.
There are a few inherited conditions that can result in kidney cancer. These are
- Von Hippel-Lindau (VHL) syndrome
- Tuberous sclerosis
- Birt-Hogg-Dube syndrome
- Hereditary non-VHL clear cell renal cell cancer
- Hereditary papillary renal cell cancer
Von-Hippel Lindau syndrome is an inherited cancer syndrome. The VHL gene runs through affected families. People who carry the gene have an increased risk of developing several quite rare cancers in the brain, spine, pancreas, eyes and inner ear. About 40% of people with VHL get kidney cancer.
Tuberous sclerosis is another condition caused by a faulty gene. About 1 in 3 cases are inherited. But the other 2 out of 3 occur because the gene has mutated in those people for the first time. It can cause skin, brain and heart problems, as well as kidney disease. People with TS have an increased risk of kidney cysts and kidney cancer. However the main tumour that they present with is a benign Angiomyolipoma (AML).
Birt Hogg Dube syndrome is another inherited condition. It causes many benign tumours to develop in the hair follicles of the skin. These usually develop on the face, neck and trunk. People that carry this gene are at increased risk of kidney cancer.
Hereditary clear cell and hereditary papillary kidney cancers are both caused by inherited faulty genes. They are dominant genetic conditions. This means that you only have to inherit the faulty gene from one parent. Even so, they are both very rare.
People with kidney cancer who have these genetic conditions often have cancer in both kidneys (bilateral kidney cancer). They may also have several tumours in each kidney. They often develop the cancer at a younger age than people with non-inherited cancers.
How do patients Present?
In its early stages, kidney cancer usually causes no obvious signs or troublesome symptoms. As a result up to 70% of kidney cancers today are found incidentally on radiological scanning being done for other reasons.
About 70% of patients present with cancer confined to the kidney (localized) or locally-advanced disease (spreading next to the kidney)
About 30% of patients present with metastases (spread of cancer to other sites) and a further third of patients develop metastases during their follow-up.
As a kidney tumor grows, symptoms may occur. These may include:
- Blood in the urine. The amount of blood may be so small that it can be detected only under a microscope or on urinalysis, a lab test often performed as part of a regular medical checkup. Less commonly the blood might be visible and discolour the urine.
- A lump or mass in the kidney area.
- Pain in the side
Other less common symptoms may include:
- Fatigue
- Fever
- Loss of appetite
- Weight loss
- Recurrent fevers
- General feeling of poor health
- High blood pressure: If the cancer interferes with the blood supply to part or all of the kidney, an enzyme called renin is released, which leads to an increase in blood pressure.
- Anaemia which results from lower than normal number of red cells in the blood.
- Recent onset varicocele in the scrotum : these are dilated veins draped around the scrotum.
- The red blood cell count may become abnormally high, resulting in a condition called polycythaemia.This is because high levels of the hormone erythropoietin produced by the tumour.
- Some people develop high levels of calcium in the blood (hypercalcemia).
Diagnosis and Staging
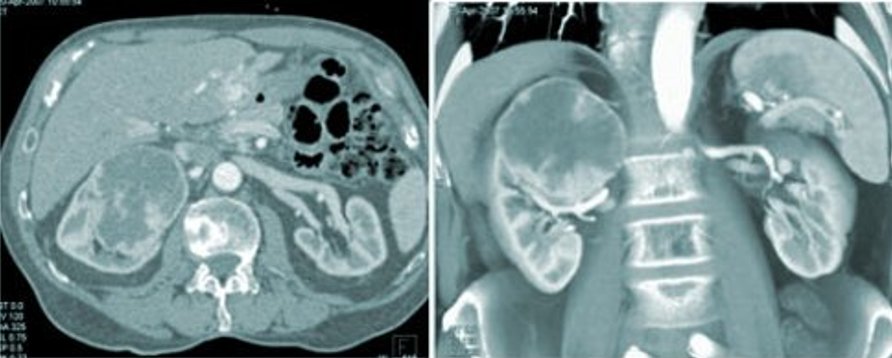
Renal tumours are found on various forms of scanning .The standard method used to find out the exact characteristics of the tumour is the CT scan. (Computerised axial Tomography)
An MRI (magnetic resonance imaging) scan will give similar information and most often one or the other will suffice.
Ultrasound or intravenous urography might have been done initially but a CT or MRI will always need to be done when a kidney tumour is suspected as they are more detailed.
If cancer is suspected to have spread beyond the kidney a Bone scan can be performed to assess whether there is any spread to the bones.
In some cases where more information is needed about the function of the kidneys a Renogram might be done.
These Radiological modalities help confirm the diagnosis but also determine the exact position of the tumour within the kidney itself and helps the decision making process regarding what surgery to perform. It helps define whether the tumour is confined to the kidney, locally advanced or metastatic. This knowledge of the tumour characteristics is called “Staging“.
Tests for Transitional Cell Cancer
If the results of scanning suggest transitional cell cancer, the urologist will likely recommend a test that examines your bladder for signs of cancer (cystoscopy). In this procedure, a long, narrow tube called a cystoscope is inserted through your urethra into your bladder. The tube carries a light source and special lens, which allow your doctor to inspect both your urethra and bladder. The cystoscope can also be used to remove a small tissue sample from a tumor. In some cases, a microscopic examination of the sediment in your urine may also help identify cancer cells.
The following are simplified definitions of the various stages of kidney cancer.
Stage T1: The primary cancer is 7 cm(about 3 inches) or less and is limited to the kidney, with no spread to lymph nodes or distant sites.
Stage T2: The primary cancer is greater than 7 cm (about 3 inches) and is limited to the kidney, with no spread to lymph nodes or distant sites.
Stage T3: The primary cancer has spread into renal veins or perinephric tissues (local area around the kidney), or to the inferior vena cava (large vein returning blood to the heart located in the middle of the abdomen near the back).
Stage T4: The cancer has spread to distant sites, invades directly beyond the local area including to the adrenal gland
Recurrent Renal Cell Cancer: Renal cell cancer has returned after primary treatment with surgery, chemotherapy, radiation or immune therapy.
Clinical stage is based on radiographic imaging before surgery, whereas pathologic stage is based on the analysis of surgically removed tissue. Staging the cancer helps predict prognosis and survival.
Physicians further denote the stage of a cancer according to a system developed by the American Joint Committee on Cancer (AJCC). This staging system includes the following criteria:
- the Size or extent of the primary kidney tumor growth into the kidney or T stage
| Primary Tumor Stage (T stage) | Graphic Representation | Description |
| T1 | 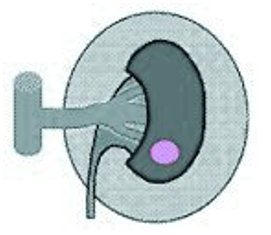 | Tumour is confined to the kidney (i.e. no penetration through the capsule) and is7 cm or less in greatest dimension |
| T2 | 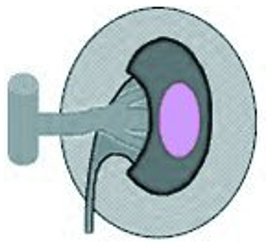 | Tumour is confined to the kidney (i.e. no penetration through the capsule) and is greater than 7 cm and less than 10cm in greatest dimension |
| T3a | 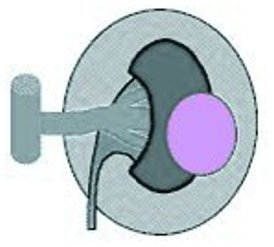 | Tumour penetrates through the kidney capsule into the pelvicaliceal system, surrounding (renal sinus or perinephric)fat, but not through Gerota’s fascia; |
| T3b or T3c | 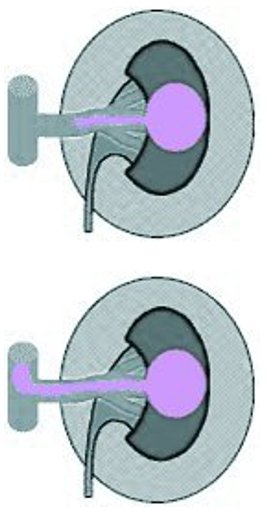 | Tumour extends into the renal vein or into the vena cava. -T3b indicates that the tumor thrombus does not extend above the level of the chest diaphragm. -T3c indicates that the tumor thrombus extends above the level of the chest diaphragm. |
| T4 | 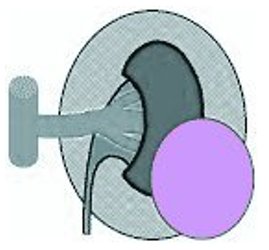 | Tumour penetrates through Gerota’s fascia. |
- the Status of Lymph Nodes near the kidney or N stage (in renal cell cancer the lymph nodes near the kidney are referred to as regional lymph nodes); and
| Regional Lymph Nodes (N stage) | Discription |
| NO | No cancer in the lymph nodes |
| N1 | Cancer in a single lymph node |
| N2 | Cancer in more than one lymph node |
- the presence or absence of cancer spread to distant sites (Metastases) or M stage
| Distant Metastasis (M Stage) | Discription |
| M0 | No metastasis |
| M1 | Distant metastasis present |
In general, cancers with higher T stage, lymph node metastasis (N stage) or distant metastasis (M stage) are worse associated with a worse prognosis and typically shorter survival periods.
Does one need a biopsy?
Kidney cancer is one of the few cancers where a biopsy is not always necessary. This is because the radiological appearance on CT or MRI scan is so characteristic that a diagnosis is possible without needing to have a tissue sample.
There are risks of getting a result of a negative biopsy when in fact cancer is present. This might lure one into thinking treatment is not indicated when in fact it might be essential. (The literature describes this in 20- 40% of cases!) There is also a risk of bleeding as it is an invasive investigation.
Probably the most common reason to do a biopsy would be if a patient had another cancer and presented with a mass in the kidney. One would then like to know if the lump was a new kidney cancer or a spread from the other cancer. Also sometimes an inflammatory mass in the kidney can look like a tumour and a biopsy would be helpful to exclude that.
It is becoming more popular to biopsy small renal masses as they might be benign and not need treatment.
It is common to biopsy patients who have masses found in both kidneys.